

PAGE AND ADDITIONAL VISUALS ARE CURRENTLY BEING ADDED.
Introduction
The Dunning-Kruger effect has long served as a cornerstone in our understanding of how individuals perceive their own competence. However, as our understanding of expertise development evolves, we need more sophisticated models to capture the nuances of professional development. Enter the Dunning-Kruger-Horizon (DKH) Effect, a three-dimensional expansion of the classical theory that adds crucial depth to our understanding of competence development.
The Three Dimensions Explained
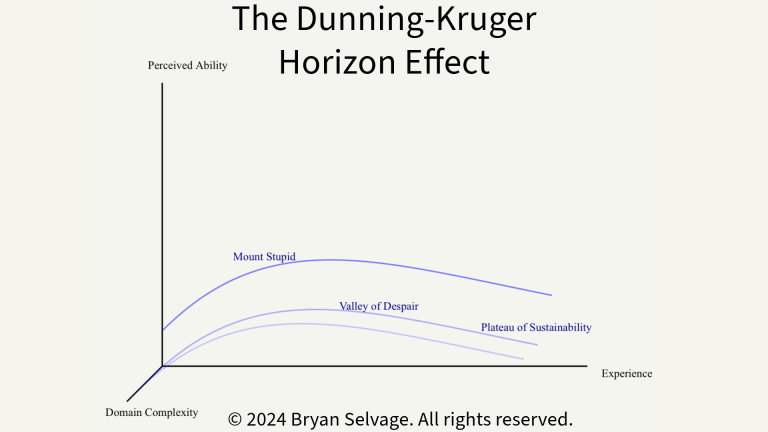
- Experience Axis (X): The traditional measure of time spent and knowledge acquired in a field
- Perceived Ability Axis (Y): How capable an individual believes they are
- Domain Complexity Axis (Z): The inherent complexity and stakes of the field being mastered
This third dimension, Domain Complexity, transforms our understanding from a simple curve into a dynamic surface that better reflects the reality of professional development. The model reveals that the journey to expertise isn’t just about accumulating experience and managing confidence—it’s about navigating increasingly complex layers of knowledge and responsibility.
Core Principles of the DKH Effect
1. The Complexity Gradient
As domain complexity increases, several key changes occur:
- Initial confidence peaks (“Mount Stupid”) become less pronounced
- The “Valley of Despair” becomes deeper and longer
- The path to genuine expertise takes longer to traverse
2. The Horizon Principle
Named for the way expertise seems to recede like a horizon as one advances, this principle suggests that in highly complex domains, even experts maintain a healthy uncertainty about their capabilities. This explains why seasoned professionals often express more measured confidence than novices.
3. Stakes-Complexity Correlation
The model proposes that domains with higher stakes (where mistakes have serious consequences) naturally develop higher complexity levels, creating steeper learning curves and more pronounced competence horizons.
Application to Paramedicine: A Case Study
Paramedicine serves as a perfect illustration of the DKH Effect in action. Let’s examine how this profession maps onto our three-dimensional model:
Phase 1: Initial Training (Low Experience, Variable Perceived Ability, Emerging Complexity Awareness)
- New EMT Students
- Experience: Minimal
- Perceived Ability: Often artificially high
- Domain Complexity: Beginning to become apparent
During this phase, paramedic students often experience a relatively modest “Mount Stupid” compared to other fields. The immediate exposure to life-and-death scenarios tends to temper overconfidence more quickly than in lower-stakes professions.
Phase 2: Early Career (Growing Experience, Realistic Perceived Ability, High Complexity Recognition)
- Newly Qualified Paramedics
- Experience: Building rapidly
- Perceived Ability: Often undergoes rapid calibration
- Domain Complexity: Full recognition hits hard
This is where the 3D model really shows its value. Unlike the traditional Dunning-Kruger curve, we see that paramedics often experience multiple “valleys of despair” as they encounter new layers of complexity:
- Clinical complexity (medical knowledge)
- Situational complexity (scene management)
- Environmental complexity (working conditions)
- Emotional complexity (patient interaction)
Phase 3: Seasoned Professional (High Experience, Calibrated Perceived Ability, Deep Complexity Understanding)
- Veteran Paramedics
- Experience: Extensive
- Perceived Ability: Realistically high but measured
- Domain Complexity: Full appreciation
At this stage, the DKH Effect reveals something fascinating: unlike in simpler domains, experienced paramedics rarely reach a point of unwavering confidence. Instead, they develop what we might call “confident humility”—high competence paired with deep respect for their field’s complexity.
Implications for Training and Professional Development
The DKH Effect suggests several important considerations for paramedic education and ongoing professional development:
- Early Complexity Exposure
- Introduce students to domain complexity early
- Use case studies that demonstrate multiple layers of challenge
- Foster appropriate levels of confidence while maintaining safety
- Structured Complexity Navigation
- Design training programs that gradually increase complexity
- Provide support through each “valley” phase
- Acknowledge and normalize the multiple challenges of competency development
- Continuous Learning Framework
- Recognize that expertise isn’t a destination but a journey
- Maintain professional development that acknowledges all three dimensions
- Foster mentorship programs that help navigate complexity
Conclusion
The Dunning-Kruger-Horizon Effect provides a more nuanced and complete picture of professional development, particularly in high-stakes fields like paramedicine. By understanding the interplay between experience, perceived ability, and domain complexity, we can better support practitioners at all stages of their careers.
This model reminds us that true expertise isn’t just about knowing more—it’s about understanding the depth and complexity of what we do, and maintaining the humility to keep learning. In paramedicine, where lives literally hang in the balance, this understanding isn’t just academically interesting—it’s professionally essential.
References
- Dunning, D. (2011). The Dunning-Kruger effect: On being ignorant of one’s own ignorance. Advances in Experimental Social Psychology, 44, 247-296.
- Croskerry, P. (2009). A universal model of diagnostic reasoning. Academic Medicine, 84(8), 1022-1028.
- Benner, P. (1984). From novice to expert: Excellence and power in clinical nursing practice. Addison-Wesley.
- Ericsson, K. A. (2008). Deliberate practice and acquisition of expert performance: A general overview. Academic Emergency Medicine, 15(11), 988-994.
- Klein, G. (2008). Naturalistic decision making. Human Factors, 50(3), 456-460.
- Endsley, M. R. (1995). Toward a theory of situation awareness in dynamic systems. Human Factors, 37(1), 32-64.
- Dreyfus, S. E., & Dreyfus, H. L. (1980). A five-stage model of the mental activities involved in directed skill acquisition. University of California, Berkeley.
- Kahneman, D., & Klein, G. (2009). Conditions for intuitive expertise: A failure to disagree. American Psychologist, 64(6), 515-526.
- Rasmussen, J. (1983). Skills, rules, and knowledge; signals, signs, and symbols, and other distinctions in human performance models. IEEE Transactions on Systems, Man, and Cybernetics, SMC-13(3), 257-266.
- Schön, D. A. (1983). The reflective practitioner: How professionals think in action. Basic Books.
- Bond, W. F., et al. (2004). The use of simulation in emergency medicine: A research agenda. Academic Emergency Medicine, 11(4), 408-414.
- Norman, G. R., et al. (2018). The causes of errors in clinical reasoning: Cognitive biases, knowledge deficits, and dual process thinking. Academic Medicine, 93(4), 638-645.
- Croskerry, P. (2013). From mindless to mindful practice—cognitive bias and clinical decision making. New England Journal of Medicine, 368(26), 2445-2448.
- Ilgen, J. S., et al. (2012). Assessing diagnostic reasoning: A consensus statement summarizing theory, practice, and future needs. Academic Emergency Medicine, 19(12), 1454-1461.
- Kolb, D. A. (1984). Experiential learning: Experience as the source of learning and development. Prentice-Hall.