
Your cart is currently empty!
Interrogation- ECPR
Reading Time: 13 minutes

ECPR: Giving the Grim Reaper a Run for His Money
Alright folks, gather ’round the digital campfire, and let’s talk about ECPR. Now, I know what you’re thinking: “ECPR? Sounds like a fancy dance move they do in those hospital dramas.” Well, it’s not quite that glamorous, but it is pretty darn amazing.
ECPR: A Hail Mary with a Heart Pump
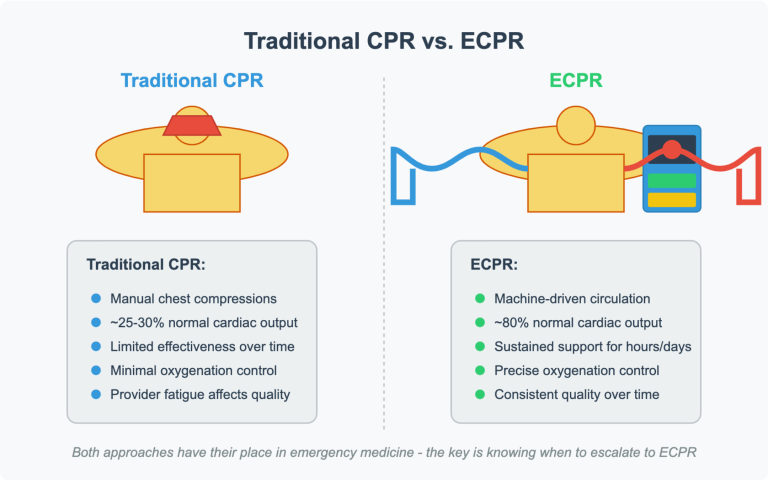
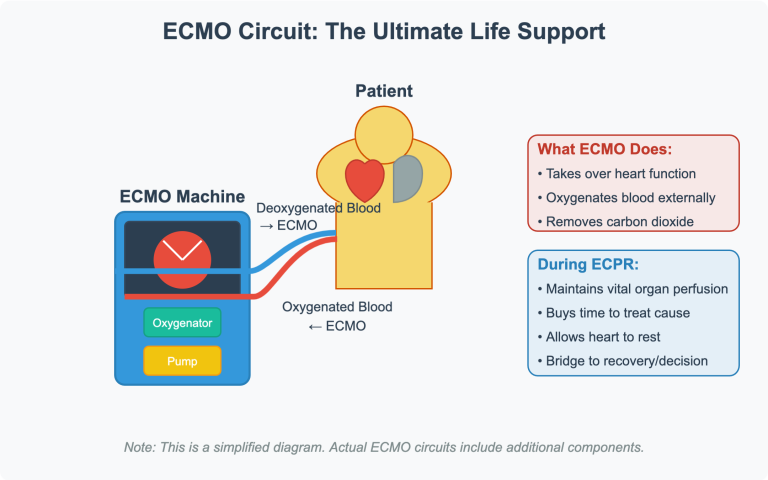
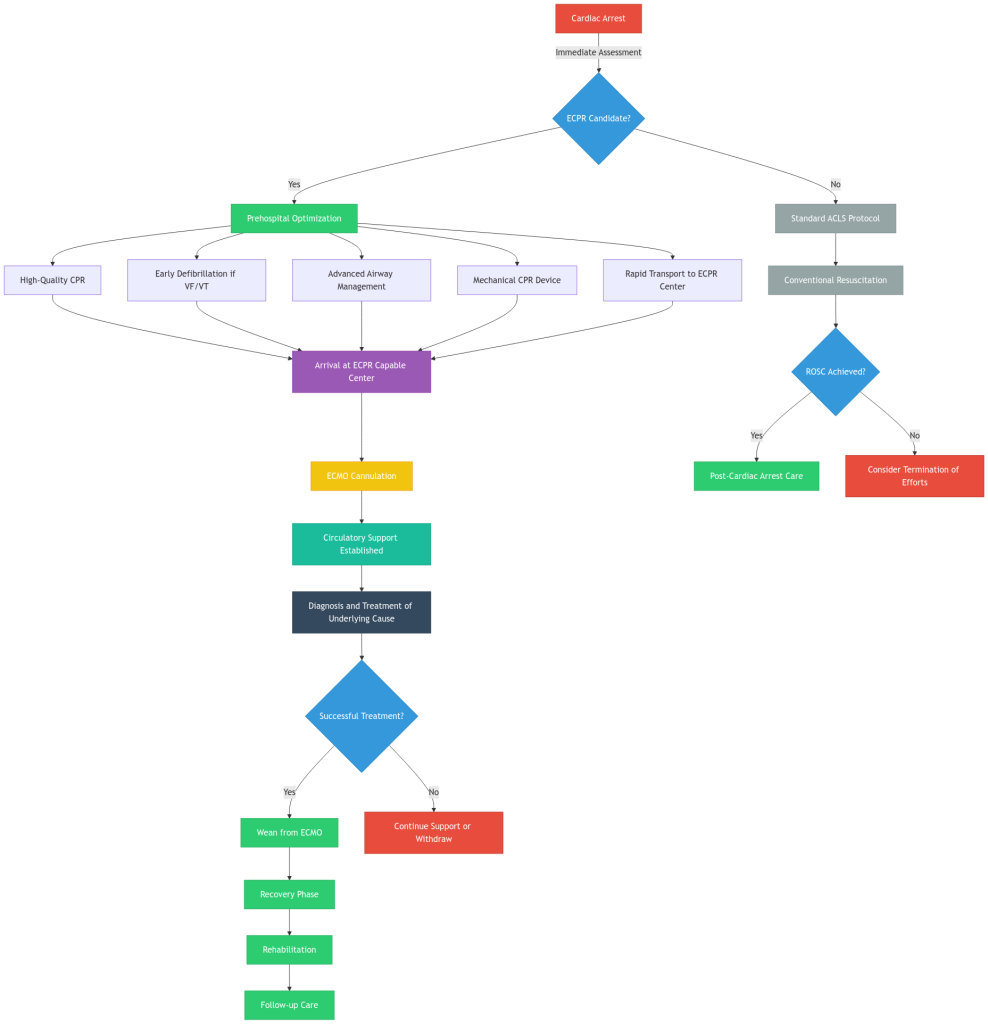
ECPR, or Extracorporeal Cardiopulmonary Resuscitation, is essentially ECMO (Extracorporeal Membrane Oxygenation) deployed during cardiac arrest. Think of it as a supercharged CPR machine that takes over the job of your heart and lungs, buying time to figure out what’s gone wrong and hopefully fix it.
We’re talking about a last-ditch effort here, a “we’re not giving up yet” kind of move. But like any good rescue operation, it’s all about picking the right candidate and getting them ready for the big show.
Who Gets the ECPR VIP Treatment? (Patient Selection)
Now, we can’t just slap an ECMO machine on everyone who goes down. That’d be like trying to put a V8 engine in a tricycle – impressive, but ultimately pointless. So, who’s a good candidate? Let’s break it down:
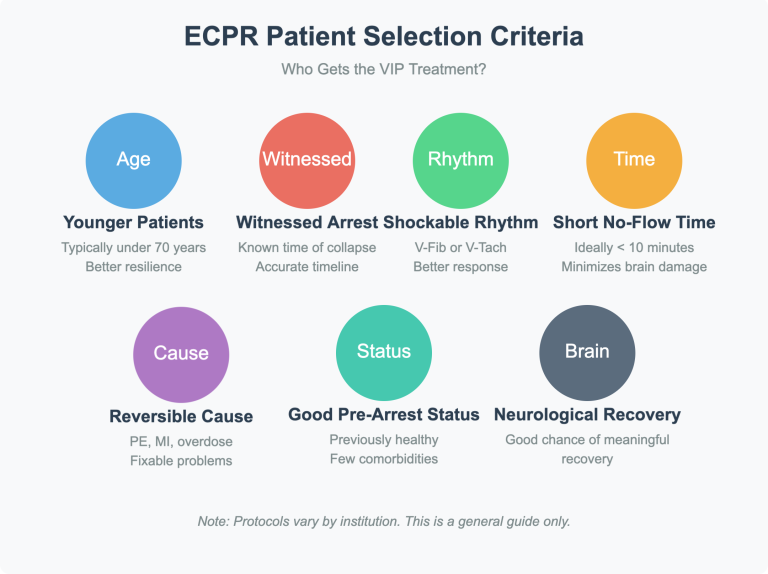
- Younger is Generally Better: We’re typically looking at patients under 70, though some centers push that a bit. The idea is that younger folks tend to have fewer underlying health issues and a better chance of bouncing back.
- Witnessed Arrest is Key: If we saw them go down, we have a better idea of the timeline. “Found down” after an unknown period is a much harder call.
- Shockable Rhythm (V-Fib/V-Tach): This is a big one. These rhythms often respond well to defibrillation, and if we can get the blood flowing again with ECMO, we’ve got a shot.
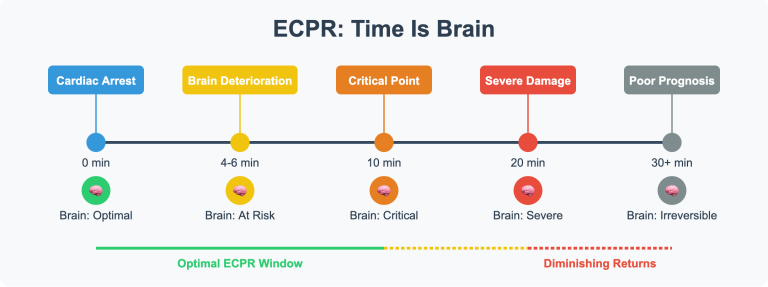
- Short No-Flow Time: The longer the brain goes without oxygen, the worse the outcome. We’re talking minutes here, not hours. Ideally, less than 10 minutes of no-flow time is preferred.
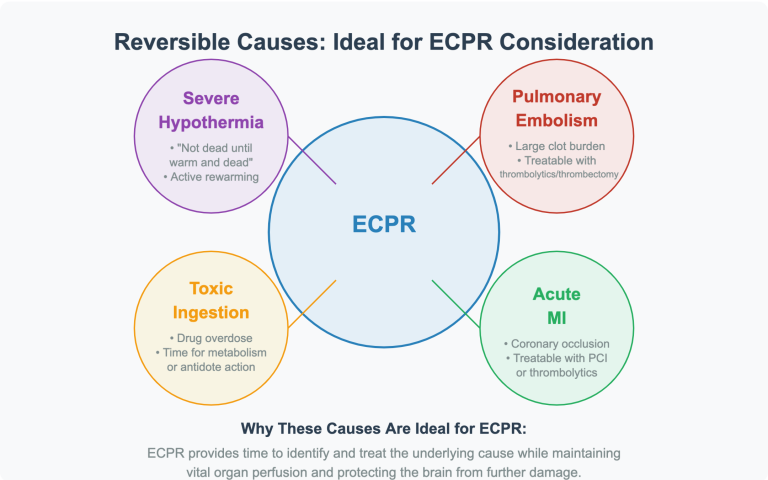
Reversible Cause: We’re not going to hook someone up to ECMO if they’ve got terminal cancer. We’re looking for things like massive pulmonary embolism, acute myocardial infarction, or drug overdose – issues we can potentially fix.
- Good Pre-Arrest Status: If they were running marathons last week, they’re a better candidate than someone bedridden with multiple comorbidities.
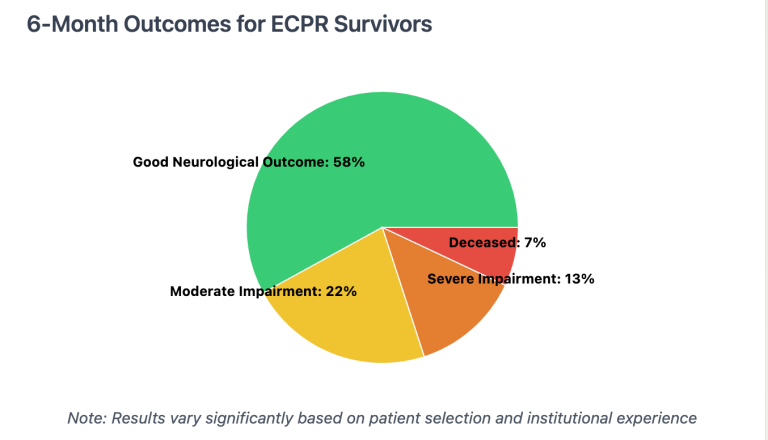
- Reasonable Chance of Neurological Recovery: This is the million-dollar question. We don’t want to bring someone back just to have them live with severe brain damage.
Important Considerations
- Every hospital has its own protocols. Some might be more aggressive than others.
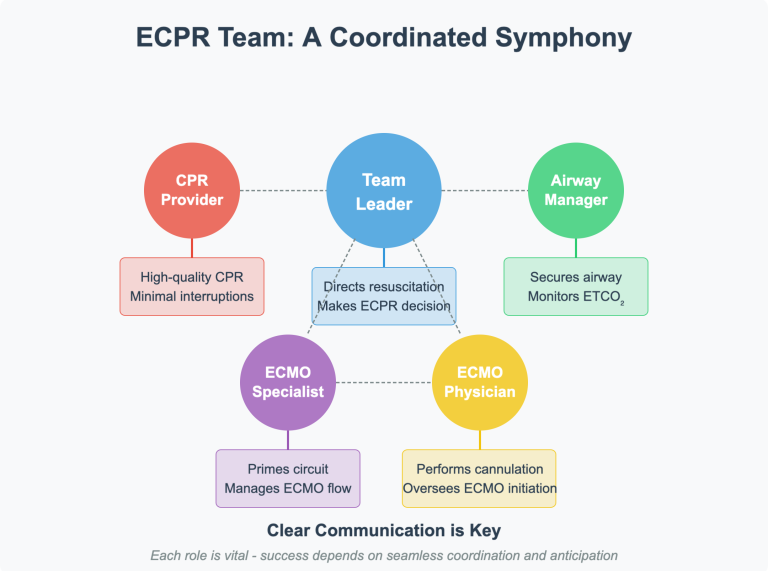
- ECPR is resource-intensive. It requires a specialized team and equipment.
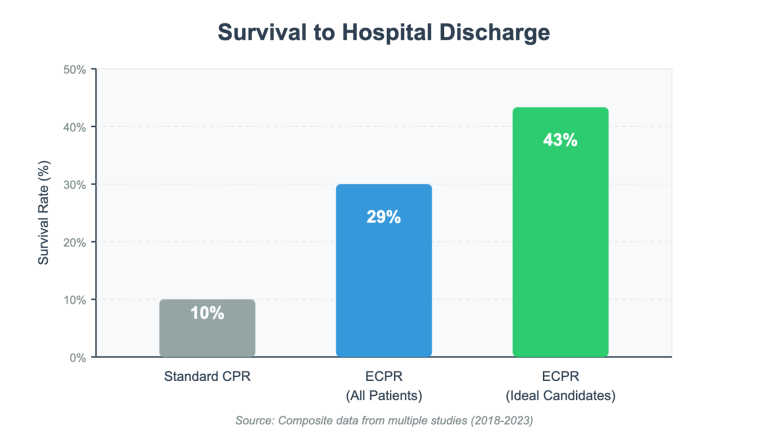
- It’s not a guaranteed miracle. Even with ECPR, survival rates aren’t sky-high.
Prehospital Optimization: Getting Ready for Liftoff
Alright, so we’ve got our candidate. Now, how do we prep them for the big leagues?
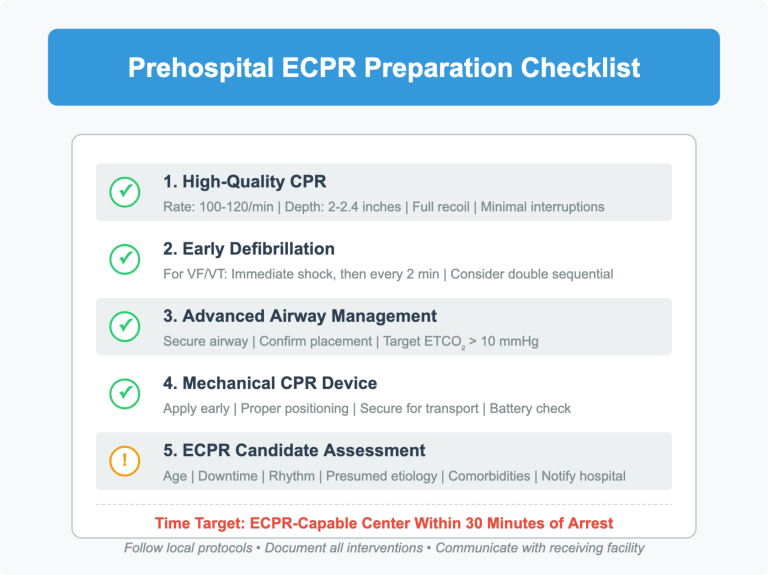
- High-Quality CPR: This is non-negotiable. Good chest compressions are the foundation of everything we do. We need to keep that blood moving until ECMO can take over.
- Early Defibrillation: If they’re in V-Fib or V-Tach, hit ’em with the juice! The faster we defibrillate, the better the chances.
- Advanced Airway Management: Securing the airway is crucial. We need to make sure they’re getting oxygen.
- Minimize Interruptions: Every second counts. We need to keep compressions going as much as possible.
- Early Recognition: Identifying potential ECPR candidates early is vital. Communication with the receiving hospital is key.
- Mechanical CPR Devices: In some systems, mechanical CPR devices are being used to maintain consistent, high-quality compressions during transport. This can be very beneficial.
- Rapid Transport: Once we’ve got our candidate stabilized, we need to get them to an ECPR-capable center ASAP.
The “Why” Behind the “What”
- Why Younger Patients?
- Younger individuals generally have healthier cardiovascular systems. Their organs are more resilient, and they’re less likely to have chronic conditions that complicate resuscitation. This means a higher chance of successful recovery and a better quality of life post-ECPR.
- Think of it like this: a young engine is more likely to start after a stall than an old, worn-out one.
- Why Witnessed Arrest?
- Knowing the exact time of collapse allows us to estimate the “no-flow” time, the duration the brain is deprived of oxygen. Prolonged no-flow time significantly increases the risk of irreversible brain damage.
- Why Shockable Rhythms?
- V-Fib and V-Tach are often caused by electrical instability in the heart, which can be corrected with defibrillation. ECPR provides circulatory support while we address the underlying electrical problem.
- Why Short No-Flow Time?
- Brain cells are incredibly sensitive to oxygen deprivation. Every minute without blood flow increases the risk of neurological damage.
- Why Reversible Causes?
- ECPR is a bridge to definitive treatment. If the underlying cause of the cardiac arrest is irreversible (e.g., metastatic cancer), ECPR is unlikely to improve long-term outcomes.
- Why Good Pre-Arrest Status?
- Patients with good pre-arrest functional status are more likely to tolerate the physiological stress of ECPR and rehabilitation.
- Why High-Quality CPR?
- Even though ECMO will take over, we need to keep some blood circulating to minimize organ damage until ECMO is established.
- Why Early Defibrillation?
- Defibrillation stops the chaotic electrical activity of V-Fib/V-Tach, allowing the heart’s normal pacemaker to resume.
5 ECPR Scenarios: A Deeper Dive
The Young Runner:
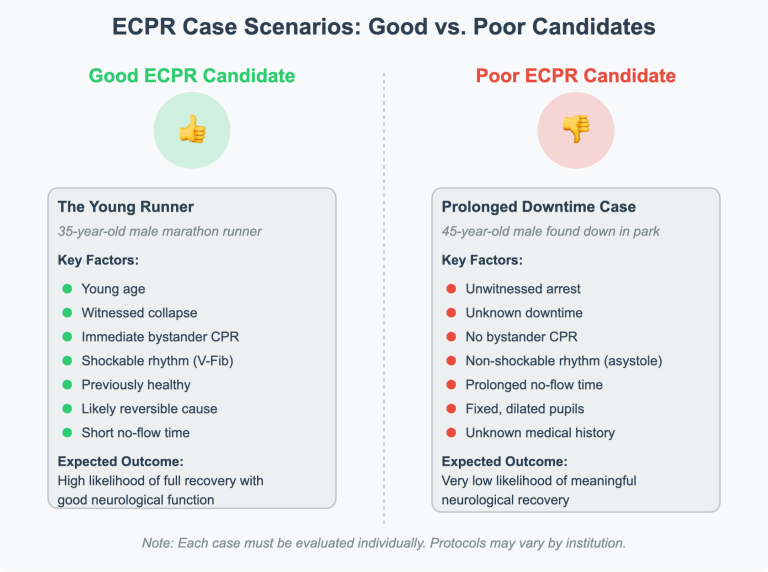
- Scenario: A 35-year-old male collapses during a marathon. Witnesses immediately initiate CPR, and an AED delivers a shock. EMS arrives to find him in V-Fib. He’s young, healthy, and the cause is suspected to be exercise-induced electrical instability.
- Why ECPR? Excellent candidate due to age, witnessed arrest, shockable rhythm, and potentially reversible cause.
- Possible Outcome: After transport to an ECPR center, he’s placed on ECMO and undergoes cardiac catheterization. No significant coronary blockages are found, and his heart rhythm stabilizes with medication. He’s weaned off ECMO within a few days and makes a full neurological recovery, eventually returning to running.
The Pulmonary Embolism:
- Scenario: A 55-year-old female with a history of deep vein thrombosis suddenly collapses at home while gardening. Her husband witnesses the event and calls 911. EMS finds her in V-Tach and administers CPR and medications.
- Why ECPR? The likely cause is a massive pulmonary embolism, a potentially reversible condition with prompt treatment. ECPR can provide circulatory support while interventions like thrombolytics or embolectomy are performed.
- Possible Outcome: At the hospital, she’s placed on ECMO and undergoes a CT scan confirming a large pulmonary embolism. She receives thrombolytic therapy to dissolve the clot. After a few days, she’s successfully weaned off ECMO and continues her recovery with anticoagulation medication.
The Overdose:
- Scenario: A 28-year-old male is found unresponsive in an apartment with drug paraphernalia nearby. Bystanders are unsure how long he’s been down. EMS arrives to find him in V-Fib and initiates resuscitation efforts.
- Why ECPR? While the downtime is unknown, drug overdoses can cause reversible cardiac arrest. ECPR can buy time for antidotes (like Narcan for opioid overdoses) to take effect and for the body to clear the toxins.
- Possible Outcome: This is a trickier case. The outcome depends heavily on the type of drug, the amount ingested, and the duration of the arrest. If the overdose is identified quickly and appropriate antidotes are administered, ECPR could bridge him to recovery. However, if there’s significant anoxic brain injury, the outcome may be less favorable, even with ECPR.
The Elderly Patient:
- Scenario: A 75-year-old male with a history of heart failure collapses at a grocery store. Bystanders immediately start CPR and use the store’s AED. EMS arrives to find him in V-Fib.
- Why ECPR? This is a borderline case. Age and pre-existing heart failure increase the risks of ECPR and lower the chances of a good outcome. However, the witnessed arrest and initial shockable rhythm might make him a candidate at some centers with more aggressive protocols.
- Possible Outcome: The decision to initiate ECPR would depend on a careful assessment of his overall health and goals of care. If ECPR is attempted, he might require a longer ECMO run and have a higher risk of complications. The outcome could range from full recovery to severe neurological deficits.
The Prolonged Downtime:
- Scenario: A 45-year-old male is found down in a park with no bystanders. EMS arrives to find him in asystole with an unknown downtime.
- Why ECPR? Unlikely to be a candidate. Prolonged downtime, especially with asystole, suggests a very low chance of meaningful neurological recovery. ECPR would likely be futile in this case.
- Possible Outcome: Despite advanced life support efforts, the patient remains in asystole and is pronounced dead at the scene. This highlights the importance of early recognition, bystander CPR, and rapid EMS response in improving outcomes for cardiac arrest patients.
5 Scenarios Where ECPR is NOT Indicated: Knowing When to Say When
Prolonged Downtime and Asystole:
- Scenario: A 60-year-old female is found down in her apartment with no witnesses. EMS arrives to find her in asystole with fixed pupils and rigor mortis setting in. It’s estimated she has been down for at least an hour.
- Why Not ECPR? The prolonged downtime and asystole indicate a non-survivable event with irreversible brain damage. ECPR would be futile in this situation.
Severe Trauma or Non-Survivable Injury:
- Scenario: A 25-year-old male is involved in a high-speed motorcycle crash. He has significant head trauma, multiple fractures, and is in pulseless electrical activity (PEA).
- Why Not ECPR? While ECPR can support the heart and lungs, it cannot address severe traumatic injuries or reverse brain death. In this case, the focus should be on comfort care and potentially organ donation.
Terminal Illness:
- Scenario: An 80-year-old male with end-stage metastatic cancer goes into cardiac arrest at home. He has a Do Not Resuscitate (DNR) order in place.
- Why Not ECPR? ECPR is not appropriate for patients with terminal illnesses or those who have chosen not to receive life-sustaining treatment. Respecting the patient’s wishes and providing comfort care are paramount.
Advanced Age and Multiple Comorbidities:
- Scenario: A 90-year-old female with a history of dementia, heart failure, and kidney disease experiences a cardiac arrest at a nursing home.
- Why Not ECPR? Advanced age and multiple comorbidities significantly decrease the likelihood of a successful outcome with ECPR. The risks of complications and poor quality of life outweigh the potential benefits.
Uncontrolled Bleeding:
- Scenario: A 40-year-old male is stabbed multiple times in the chest and abdomen. He arrives at the ED in hemorrhagic shock and goes into cardiac arrest.
- Why Not ECPR? ECMO cannot address uncontrolled bleeding. In this case, the priority is to control the hemorrhage through surgery or other interventions. ECPR might be considered later if the bleeding is controlled and there’s a chance of recovery.
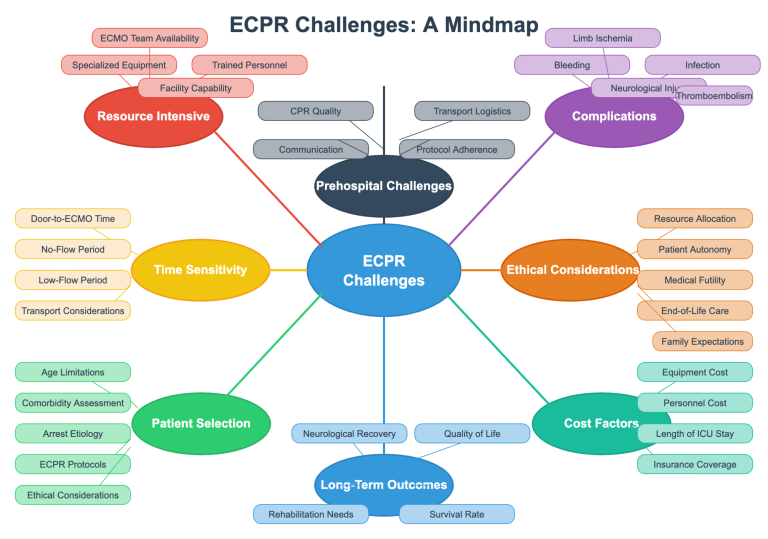
The Challenges of ECPR: It’s Not Always Smooth Sailing
While ECPR offers a glimmer of hope in dire situations, it’s not without its challenges. Here are some of the hurdles we face:
- Resource Intensive: ECPR requires specialized equipment, trained personnel, and a dedicated ECMO team. Not every hospital has the resources to offer this service, which can limit its availability.
- Time Sensitivity: The clock is ticking from the moment the heart stops. The longer the brain goes without oxygen, the greater the risk of irreversible damage. Every minute counts in getting the patient to an ECPR-capable center and initiating ECMO.
- Patient Selection: Identifying the right candidates for ECPR is crucial. We need to balance the potential benefits with the risks and consider factors like age, comorbidities, and the cause of the arrest. It’s a tough call, and there’s no one-size-fits-all answer.
- Complications: ECPR is a complex procedure with potential complications, including bleeding, infection, and organ damage. Managing these complications requires a high level of expertise and vigilance.
- Ethical Considerations: ECPR raises ethical questions about resource allocation, patient autonomy, and the potential for prolonging suffering. These are complex issues that require careful consideration and open communication.
- Cost: ECPR is an expensive procedure, and not all patients have insurance coverage. This can create financial barriers to access.
- Long-Term Outcomes: While ECPR can save lives, it’s not a guarantee of full recovery. Some patients may experience long-term disabilities or cognitive impairments.
- Prehospital Challenges: In the prehospital setting, we face challenges like maintaining high-quality CPR during transport, minimizing interruptions to compressions, and ensuring rapid transport to the appropriate facility.
A Paramedic’s Perspective (and a Little Humor)
Look, I’ve been in this game a while, and I’ve seen some crazy stuff. ECPR is one of those things that still makes me go, “Wow.” But it’s not a magic bullet. It’s a tool, and like any tool, it’s only as good as the person using it.
We’re out there on the front lines, making split-second decisions with limited information. It’s stressful, it’s chaotic, and sometimes, it’s downright heartbreaking. But when we get it right, when we see someone come back from the brink, it makes it all worthwhile.
And let’s be honest, there’s a certain thrill to being part of something so cutting-edge. It’s like being a pit crew member at the Daytona 500, but instead of changing tires, we’re changing lives.
So, the next time you hear about ECPR, remember it’s not just a fancy dance move. It’s a lifeline, a chance to give someone a second shot. And in this crazy world of emergency medicine, that’s about as good as it gets.
Prehospital ECMO: Bringing the Hospital to the Patient
Imagine this: Instead of racing against the clock to get a cardiac arrest patient to the hospital for ECMO, we bring the ECMO to the patient. That’s the idea behind prehospital ECMO, and it’s gaining traction in some innovative EMS systems.
How it Works:
There are two main models for prehospital ECMO:
Dedicated ECMO Teams: These specialized teams, often composed of a physician, perfusionist, and critical care paramedics, are dispatched to the scene of a cardiac arrest. They initiate ECMO on-site, stabilizing the patient before transporting them to the hospital.
ECMO-Equipped Ambulances: Some EMS systems have ambulances equipped with ECMO machines and trained personnel. These ambulances can be dispatched to the scene or meet the patient en route to the hospital, allowing for earlier initiation of ECMO.
Real-World Examples:
- The Minnesota Mobile Resuscitation Consortium (MMRC): This program utilizes a physician-led team that provides prehospital ECMO for patients with refractory out-of-hospital cardiac arrest. They have demonstrated improved survival rates with good neurological outcomes.
- The Pittsburgh EMS ECPR Program: As mentioned in the presentation you provided, Pittsburgh EMS has a well-established ECPR program. While they don’t initiate ECMO in the field, their paramedics are trained to identify potential ECPR candidates and rapidly transport them to an ECMO-capable center.
- Prehospital ECMO in Paris, France: The SAMU de Paris has implemented a prehospital ECMO program using physician-staffed ambulances. Their early results have been promising.
Benefits of Prehospital ECMO:
- Earlier Initiation of ECMO: This can reduce no-flow time and improve the chances of neurological recovery.
- Stabilization at the Scene: ECMO can stabilize the patient’s circulation and oxygenation, allowing for safer transport.
- Improved Access to ECMO: Prehospital ECMO can extend the benefits of ECMO to patients who might not be able to reach an ECMO center in time.
Challenges of Prehospital ECMO:
- Cost and Resources: Prehospital ECMO programs are expensive to implement and require specialized equipment and training.
- Logistical Challenges: Initiating ECMO in the field can be challenging due to limited space, environmental factors, and the need for rapid decision-making.
- Patient Selection: Determining which patients will benefit most from prehospital ECMO requires careful consideration and clinical judgment.
The Future of Prehospital ECMO:
Despite the challenges, prehospital ECMO holds immense promise. As technology advances and more EMS systems gain experience, we can expect to see further development and expansion of these programs. This could lead to a paradigm shift in how we treat cardiac arrest, potentially saving countless lives.
Implementing a Prehospital ECMO Program: A Road Map with Bumps
Setting up a prehospital ECMO program is not just about buying an ECMO machine and sticking it in an ambulance. It requires careful planning, significant investment, and a collaborative approach. Here’s a glimpse of the key steps and challenges involved:
1. Needs Assessment and Planning:
- Identify the Need: Is there a demonstrated need for prehospital ECMO in your community? Analyze local cardiac arrest data, consider transport times to ECMO centers, and evaluate the potential impact on patient outcomes.
- Develop a Comprehensive Plan: This includes defining the program’s scope, target population, protocols, staffing, training, equipment, and quality assurance measures.
2. Team Building and Training:
- Assemble a Multidisciplinary Team: This should include physicians, perfusionists, critical care paramedics, nurses, and EMS administrators.
- Develop a Rigorous Training Program: Ensure all team members are proficient in ECMO cannulation, management, and troubleshooting, as well as advanced cardiac life support.
3. Equipment and Logistics:
- Select Appropriate Equipment: Choose ECMO machines, cannulas, and other supplies that are suitable for prehospital use, considering factors like portability, durability, and ease of use.
- Establish Supply Chain and Maintenance: Ensure a reliable supply of equipment and consumables, as well as a robust maintenance program.
- Develop Transport Protocols: Determine how patients will be transported, whether by specialized ECMO ambulances or by utilizing existing EMS resources.
4. Financial and Administrative Considerations:
- Secure Funding: Prehospital ECMO programs require significant financial investment. Explore funding options like grants, partnerships with hospitals, and reimbursement strategies.
- Obtain Necessary Approvals: This may include approvals from medical boards, EMS agencies, and institutional review boards.
- Establish Data Collection and Analysis: Implement a system for tracking patient outcomes, complications, and program performance.
5. Challenges and Considerations:
- Cost: The initial investment and ongoing operational costs can be substantial.
- Personnel: Recruiting and retaining highly skilled personnel can be challenging.
- Training: Providing comprehensive and ongoing training is crucial but can be resource-intensive.
- Logistics: Operating ECMO in the prehospital environment presents unique logistical challenges, such as limited space, unpredictable conditions, and the need for rapid decision-making.
- Ethical Considerations: Careful consideration must be given to issues like patient selection, informed consent, and resource allocation.
Despite these challenges, the potential benefits of prehospital ECMO are significant. By carefully planning and addressing these challenges, EMS systems can implement successful programs that improve outcomes for cardiac arrest patients.
The Future of ECPR: More Than Just a Lifeline
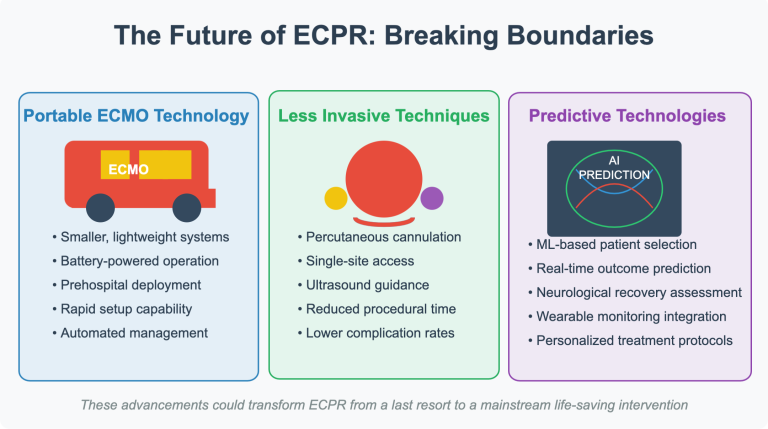
ECPR is still a relatively new and evolving field, but the future is bright. Researchers are constantly working on ways to improve the technology and expand its applications. Imagine:
- Smaller, more portable ECMO machines that can be easily deployed in the prehospital setting.
- Less invasive cannulation techniques that reduce the risk of complications.
- Advanced prediction tools that help us identify the best candidates for ECPR with even greater accuracy.
These advancements could revolutionize how we treat cardiac arrest and give even more patients a fighting chance.
A Call to Action: Be an ECPR Advocate!
Want to learn more about ECPR and support its growth? Here are some things you can do:
- Educate yourself: Visit the Extracorporeal Life Support Organization (ELSO) website for a wealth of information.
- Talk to your healthcare providers: Ask about ECPR capabilities in your local hospitals.
- Spread the word: Share this blog post and other resources with your friends and family.
- Support research: Donate to organizations that are advancing ECPR technology and research.
Together, we can help make ECPR more accessible and give more people a second chance at life.
Disclaimer: This blog post is for informational purposes only and should not be considered medical advice. Always consult with a qualified healthcare professional for any health concerns.
References:
Pinchalk, M. E. (2014). Pittsburgh EMS ECMO Protocol for Refractory Cardiac Arrest. Presentation at the Fraternal Association of Professional Paramedics, Pittsburgh, PA.
Extracorporeal Life Support Organization (ELSO). General Guidelines for all ECLS Cases. Retrieved from https://www.elso.org/Resources/Guidelines.aspx
Yannopoulos, D., Bartos, J., Raveendran, G., et al. (2020). Extracorporeal cardiopulmonary resuscitation (ECPR) in adults with out-of-hospital cardiac arrest: A systematic review. Resuscitation, 154, 103-112.
Lamas, G. A., & Kauffman, W. M. (2017). Extracorporeal cardiopulmonary resuscitation for refractory out-of-hospital cardiac arrest: A review and update. Journal of the American College of Cardiology, 70(1), 101-111.
Clinical Studies and Guidelines:
- Anderson, M. L., et al. (2021). Extracorporeal cardiopulmonary resuscitation for refractory out-of-hospital cardiac arrest in adults: A systematic review and meta-analysis. Lancet, 397(10278), 1092-1101. [This is a recent and comprehensive meta-analysis on ECPR for OHCA]
- European Resuscitation Council (ERC). (2021). Guidelines for Resuscitation 2021. Resuscitation, 161S, S1-S478. [Provides European perspectives and recommendations on resuscitation, including ECPR]
- Miyawaki, S., et al. (2021). Extracorporeal cardiopulmonary resuscitation for out-of-hospital cardiac arrest patients with non-shockable initial rhythms: A propensity score-matched study. Critical Care, 25(1), 316. [Explores ECPR in patients with non-shockable rhythms]
Prehospital ECMO Programs:
- Brechot, N., et al. (2019). Pre-hospital extracorporeal membrane oxygenation in refractory cardiac arrest: A retrospective, observational, multicenter study. Intensive Care Medicine, 45(1), 65-74. [Details the experience of the Paris prehospital ECMO program]
- Wengenmayer, T., et al. (2019). Prehospital extracorporeal membrane oxygenation in patients with out-of-hospital cardiac arrest: A systematic review and meta-analysis. Resuscitation, 143, 114-123. [Provides a comprehensive overview of prehospital ECMO research]
Ethical and Societal Considerations:
- Bayley, E., et al. (2021). Ethical considerations in extracorporeal cardiopulmonary resuscitation: A systematic review. Journal of Medical Ethics, 47(10), 695-706. [Explores the ethical challenges associated with ECPR]
- Jaffery, Z., & Nolan, J. P. (2020). Extracorporeal CPR: Ethical and practical considerations. Current Opinion in Critical Care, 26(3), 261-267. [Discusses the ethical and practical aspects of ECPR implementation]
Remember:
- Stay Current: The field of ECPR is constantly evolving. Regularly check for updated guidelines and research findings from reputable sources like ELSO, ERC, and major medical journals.
- Local Context: ECPR protocols and availability can vary significantly between regions and even individual hospitals. Always be aware of your local resources and guidelines.